- 07914803818
- 02077940500 ext: 34273
- mvarcada.practice@nhs.net
Crohn's disease is a chronic inflammatory bowel disease. Inflammatory means that the body's own immune system is attacking the digestive tract anywhere from the mouth to the anus, though usually it attacks areas in the small and large intestines. It usually develops in the late teens/early 20s or in the 50-60 age group. If managed, the disease can be controlled and hopefully prevented from relapsing, though there is currently no cure.
What causes Crohn's?
There is no known single definitive cause for Crohn's disease. As far as we currently know, it is caused by an interaction between your genes, the environment, your lifestyle (eg. smoking) and natural variants in your immune system. Research is still ongoing into finding more answers.
What complications are there?
As Crohn's is a chronic condition, a relapse may happen at any point. This may be evident with a return to your original symptoms, which may include diarrhoea, abdominal pain, weight loss, loss of appetite, and even blood in your stools. You will need to see your GP if you have a relapse. Crohn's can also affect areas other than the digestive tract. You may get sore, red eyes, painful joints, and unusual rashes on your skin. In addition, the disease can cause complications in and around the anus. You can get something called a fissure, which is a crack in the skin around the anus, which can bleed. You may also develop fistulae, which are abnormal connections between the digestive tract and the outside. Although unpleasant, these can be treated. Abscesses and piles may also develop.
How is Crohn's disease treated?
There are two goals to managing Crohn's disease. First the disease is brought under control so it doesn't affect you as much (inducing remission) and then you aim to keep it that way (maintaining remission). One of the most important things to do is stop smoking. Services to assist this are available at your GP or at your hospital.
Inducing remission: To bring Crohn's under control after a flare, or when first seen by a doctor, a steroid will be used, usually in tablet form, but possibly by a drip into your veins. Side effects of this treatment can include acne and mood changes, but these will not be permanent as you will be slowly taken off the steroid. There may be an option for surgical removal of the bowel however this is not a cure.
Maintaining remission: To keep your disease under control, there are a variety of options that your doctor will discuss with you. Most people will be on either Mercaptopurine or Azathioprine. It is important to carry on taking these if you start, as stopping increases the chances of relapse. Other drugs, such as Infliximab, are available, though not usually the first choice treatment. If you have had surgery then your doctor may suggest that you take one of the above drugs. Even if you choose not to receive treatment, your doctor will continue with check-ups and monitor your disease.
Crohn's disease and Cancer Another type of inflammatory bowel disease, Ulcerative Colitis, is associated with an increased risk of bowel cancer. However, as Crohn's can affect all over the digestive tract, the risk of cancer varies. If your small bowel is mainly affected, then it is unlikely to increase your risk of cancer. If it affects the large intestine extensively, often called Crohn's colitis, then the risk increases after 20 years of disease to 7 in 100 people (compared to 5 in 100 of the general population).
Crohn's and Pregnancy It is important that you talk to your doctor if you are hoping to conceive. Many people with Crohn's have gone on to have healthy children, but there are important things to consider. One of these for women is that if your disease is active, it may be harder to conceive. Most doctors will advise having your disease under control before trying to conceive, as it can complicate pregnancy. Some medications may also have side effects upon your baby, so it is best to discuss this with your doctor.
Ulcerative colitis is an intermittent form of inflammatory bowel disease affecting the rectum and often extending into the colon. It is currently thought that usually harmless bacteria can cause a reaction in certain individuals, leading to their colon becoming inflamed. The reason this affects some people but not others is not fully understood.
Who does ulcerative colitis affect?
Ulcerative colitis usually begins between 15 and 30 years of age, and it can affect men and women equally. Approximately 100,000 people in the UK are affected by ulcerative colitis.
What are the symptoms?
The three most common symptoms are: diarrhoea bleeding from the back passage abdominal pain Not everyone will experience all three symptoms at once; for example some patients may only notice they pass blood when opening their bowels. Patients may also experience some weight loss and fevers. Occasionally the inflammation in ulcerative colitis can affect other parts of the body, such as the joints or skin.
What is a colonoscopy and why do I need one?
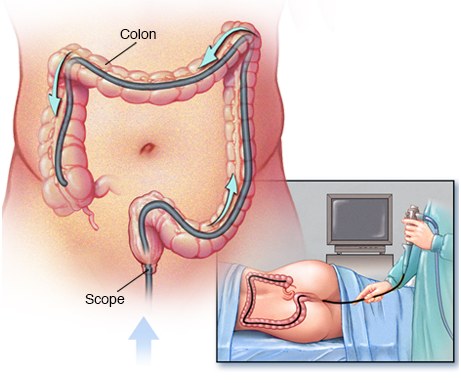
A colonoscopy is an examination with a camera on a flexible tube that is inserted into the back passage, usually you are sedated. With this it is possible to see the rectum and the entire colon.
Your doctor may take a few biopsies during this procedure (small samples of the bowel lining). With this it is possible to diagnose ulcerative colitis as well as seeing the extent of disease. Individuals with long-term ulcerative colitis are also at a slightly increased risk of bowel cancer, so a colonoscopy can be performed to look for any early signs of disease.
What treatment options are available?
Anti-inflammatory medication may come as a suppository or as tablets. Although suppositories may seem unpleasant, they ensure the medication gets directly to the site of disease and are useful when only a small amount of the colon is affected. If the inflammation is severe, you may be given steroids. These are reserved for severe cases because they come with more side effects.
Some anti-inflammatory treatments are also given when the disease is inactive to prevent relapse.
What if medication fails?
If ulcerative colitis fails to respond to treatment, or patients become very unwell, a surgical operation to remove some or the entire colon is considered, called a colectomy.
Removal of the colon prevents it becoming inflamed, so treats the disease. This procedure previously required the patient to need a colostomy bag on their abdomen, but instead nowadays part of the small intestine can usually be made into a pouch which acts as the rectum, meaning a colostomy bag is not needed.
Microscopic colitis is a condition that causes watery diarrhea. It involves the colon, which is another name for the large intestine. There are 2 types of microscopic colitis, lymphocytic colitis and collagenous colitis. Both types cause the same symptoms and are treated the same way.
Who gets microscopic colitis?
Microscopic colitis happens when the colon gets inflamed. But doctors don't always know what makes the colon inflamed. In some cases, the condition seems to be caused by an infection in the digestive system. In other cases, it seems to be caused by medicines. For example, a group of medicines called non-steroidal antiinflammatory drugs, or "NSAIDs" for short, sometimes causes microscopic colitis.
What are the symptoms of microscopic colitis?
Microscopic colitis causes episodes of diarrhoea that is watery and not bloody. Most people have 4 to 9 watery bowel movements a day, but some people have more. Diarrhoea can last weeks to months.
People sometimes have other symptoms, too. These commonly include weight loss, belly pain, or feeling very tired.
Test for microscopic colitis:
Your doctor or nurse will do an exam and order different tests to exclude other causes of diarrhoea and diagnose microscopic colitis. These can include:
- Blood tests
- Lab tests on a sample of your bowel movement
Colonoscopy – This is a procedure that lets the doctor look at the inside of your colon. During a colonoscopy, the doctor will do a test called a biopsy and he will take small samples of tissue from your colon. A biopsy is the only test that can tell for sure whether you have microscopic colitis.
Treatment
Treatment depends on your individual situation. It usually involves one or more of the following:
Medicine changes – If your doctor thinks that your symptoms are caused by a medicine you take, he or she will recommend that you stop taking that medicine.
Anti-diarrhoea medicines, such as loperamide (brand name: Imodium) These medicines reduce the number of bowel movements you have.
A steroid medicine called budesonide. This is different from the steroids athletes take to build muscle. This medicine helps reduce inflammation in the colon.
If these treatments don't help enough to ease your symptoms, let your doctor or nurse know. There are other medicines or treatments that might help.
Some people need to be on treatment long term. That's because symptoms sometimes come back after treatment is stopped.
High likelihood |
Intermediate likelihood |
Low likelihood |
Acarbose |
Carbamazepine |
Cimetidine |
Aspirin and NSAIDs |
Celecoxib |
Gold salts |
Clozapine |
Duloxetine |
Piascledine |
Entocapone |
Fluvastatin |
|
Flavonoid* |
Flutamide |
|
Proton pump inhibitors |
Oxetorone |
|
Ranitidine |
Madopar |
|
Sertraline |
Paroxetine |
|
Ticlopidine |
Simvastatin |
|


